One of the basic lessons of Twitter is to make your tweet ideally ‘visually eye catching’. Hence, a stunning photo might help.
It’s often said that you must make sure that ‘your content is not caught in a timewarp‘. By this, marketing professionals provide that your promotion must relate to the current configuration of a product, not, for example, a prototype.
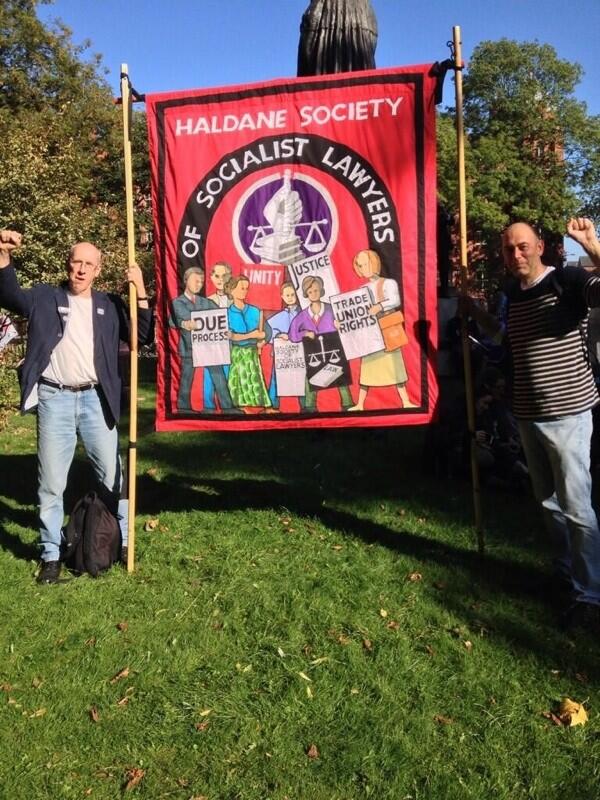
Two Labour MPs literally decided to tweet about the #NHS299 protest outside #cpc13 by showing the same image of the ‘Stop the War’ protest against a Labour government from a few years ago.
Around 60,000 arrived today in Manchester for the first day of the Conservative Party conference to protest against austerity cuts and NHS changes. There was not a single arrest, at the time of publication of this blogpost.
The central accusation is that the executive members of the Conservative Party were able to legislate, with the help of Liberal Democrat votes, in the House of Commons and House of Lords for an act of parliament which made it very easy for contracts to be awarded to the private sector not the NHS or public sector. The cap allowed for income to be generated privately was massively uplifted.
It is specifically proposed that both legislative measures allowed the privatisation of the NHS through effectively outsourcing it. Andy Burnham MP, Shadow Secretary of State, has described this as making the NHS more like the US market, and has promised many times to reverse the marketisation and to repeal the Health and Social Care Act (2012). The ‘National Hospital Sell-Off’ (NHS), as it has now become described, was tweeted today by Burnham today to be “now advancing like a juggernaut. In last year alone, 81 major contracts – worth £4.5 billion – put out to market. #nhs299“.
The march set off at midday and passed through the centre of the city. It will end with speeches at a rally in Whitworth Park. Greater Manchester Police said that the mile long protest was one of the largest they had ever watched over, and that no arrests have been made.
Frances O’Grady, TUC general secretary, said beforehand: “The march and rally will allow thousands of ordinary people to show the government exactly what they think of their policies. Austerity is having a devastating effect on our communities and services, with 21,000 NHS jobs lost over the last three months alone. The NHS is one of Britain’s finest achievements and we will not allow ministers to destroy, through cuts and privatisation, what has taken generations to build.” Burnham has further embellished the central accusation by saying the biggest NHS ‘top down reorganisation’, not democratically called for, put profit before people.
As the march set off at noon, UNISON general secretary Dave Prentis was joined by Andy Burnham MP and health workers from George Eliot Hospital in Nuneaton, which is under threat of privatisation. Campaigners ensured that Twitter hashtag #NHS299 was trending right across the UK – emphasising the importance of the news, but getting the message across in the national media was exceptionally difficult due to lack of coverage from the BBC. 90 minutes after the first marchers had moved off, coaches were still reported to be arriving in Manchester, with the official Twitter account for the demonstration reporting that the front section was “holding at Albert Square for a bit to allow people to catch up”.
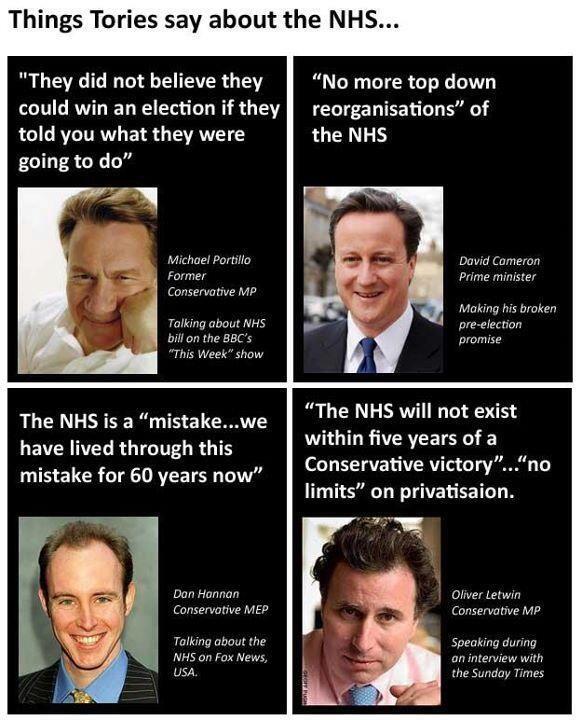
But we don’t just need to improve the health service, friends; we’ve got to rescue it from these Tories. And the Liberals too. Now look, before the election, I remember the speeches by David Cameron. I remember one where he said the three most important letters to him were NHS. Well he has got a funny way of showing it, hasn’t he? And when they came to office, they were still saying how brilliant was in the health service, how the health service was doing great things and the doctors and nurses and so on. Now have you noticed they have changed their tune recently? Suddenly they are saying how bad everything is in the NHS. Now the vast majority of doctors and nurses do a fantastic job. Sometimes things go wrong. And when they do, we should be the first people to say so. But hear me on this. The reason David Cameron is running down the NHS is not because the doctors and nurses aren’t doing as good a job as they were before. It is because they have come to a realisation that the health service is getting worse on their watch and they are desperately thrashing around trying to find someone else to blame. Blame the doctors, blame the nurses, blame the last Labour government. That is what they are doing. Well let me tell you about the record of the last Labour government. When we came to office there were waiting time targets of 18 months that were not being met, when we left office there were waiting time targets of 18 weeks that were being met. When we came to office there was an annual winter A&E crisis, when we left office the people had A&E services they could rely on. When we came to office there were fewer doctors and nurses, we when left office more doctors and nurses than ever before. And when we came to office people said well the health service, it was a good idea in previous generations but I don’t really believe it will be there in the next, and we left office with the highest public satisfaction in the history of the health services. Yes friends, we did rescue the National Health Service. So when you hear David Cameron casting arou nd for someone to blame for what is happening in the NHS just remember it is not complicated, it’s simple, it’s as simple as ABC: when it comes to blame, it is Anyone But Cameron. We know who is responsible, the top-down reorganisation that nobody voted for and nobody wanted, the abolition of NHS Direct, the cuts to social care, the fragmentation of services. We know who is responsible for thousands of fewer nurses, we know who is responsible not just for an annual A&E crisis, but an A&E crisis for all seasons. It is this Prime Minister who is responsible. So friends it is the same old story, we rescue the NHS, they wreck the NHS and we have to rescue it all over again. And that is what the next Labour government will do.
Addicts are great customers, they have a huge appetite for your product and they keep coming back.
That of course is the market-driven view of public health. A coherent national public health policy should consider the evidential impact of measures on the health of its citizens.
The last few years have indeed seen a public health which appears to have been somewhat determined by the phenomenon of ‘corporate capture’, such as the interests of corporates rather than public health physicians. This is of course partly a reflection of the current government in office, and spans across a growing number of policies including obesity, packaging of cigarettes, and pricing of alcohol.
A buzzword in management circles has been ‘disruption‘. It is felt that early digital cameras suffered from low picture quality and resolution and long shutter lag. Quality and resolution are no longer major issues and shutter lag is much less than it used to be. The convenience and low cost of small memory cards and portable hard drives that hold hundreds or thousands of pictures, as well as the lack of the need to develop these pictures, also contributed to the successful adoption of these disruptive technologies. Digital cameras have a high power consumption (but several lightweight battery packs can provide enough power for thousands of pictures).
According to Wikipedia, a disruptive innovation “is an innovation that helps create a new market and value network, and eventually goes on to disrupt an existing market and value network, displacing an earlier technology”. It is a term used to describe changes that improve a product or service in ways that the market does not expect.
Disruptive technologies have created new industries and new markets. They have also rendered others obsolete and outdated. They provided consumers with something they did not know they wanted. The economist Joseph Schumpeter referred to this process as “creative destruction.” Early investors in these companies certainly took on a lot of risk. There was no way to know whether or not an idea would be profitable. After all, these ideas had no track record.
The American investment banking firm Goldman Sachs earlier this year released a list of eight disruptive themes that have the potential to reshape their categories and command greater investor attention in the near future. Electronic cigarettes were listed as one of these eight markets investors should keep an eye on, for their potential to transform the tobacco industry.
The little vaping companies that make alternative devices may not make it into the fortune 500 or onto the boards of the NYSE, but they will survive because they have a passionate clientele. They’re like the little mammals that scurried around the massive feet of the dinosaurs at the end of the Jurassic, 65 million years ago, just as the big guys were about to go belly up. Bet on the little guys. They’ll survive.
On October 8th 2013, the European Parliament is to vote on a proposal to regulate the devices as if they were medical products. E-cigarettes (“e-cigs”), which allow users to inhale nicotine-laced vapour instead of tar-clogged smoke, are a growing market, set to top $1bn in the next three years. Smoking is falling in most rich countries, but “vaping” is rising. In Europe, 7m people are thought to be using e-cigs, which vaporise a solution containing nicotine without the toxins from burning tobacco. Sales of e-cigs in America may treble this year, according to figures from Bonnie Herzog of Wells Fargo, a bank. She thinks their consumption could overtake that of ordinary cigarettes in a decade.
An “e-cig” is composed of a mouthpiece, a liquid nicotine cartridge, a heating element and a battery. When the user inhales on the e-cig, the heating element is activated. The liquid nicotine cartridge is heated and creates a vapor. This is what the user inhales. It is odourless. It doesn’t contain any of the other chemicals or tar found in traditional cigarettes.
E-cigs may be far safer than normal cigarettes and at least as good at getting people to quit smoking as nicotine patches and gum, but they too are based on that addictive substance. Manufactured by hundreds of suppliers using materials from China and elsewhere, the quality and labelling of e-cigs on sale are known to be uneven.
E-cigs can be smoked indoors. Once again, there are no noted effects of secondhand vapour. The vapour that is exhaled has little to no odour. Bar and club owners may even be becoming fans of e-cigs. Users who buy them are more likely to stay in the bar and consume more drinks than they otherwise would. This may add to the ‘coolness’ and convenience factor of these disruptive new products. There are a number of possible suggested benefits.
There is a noted reduction in side effects commonly reported by smokers. Some of these side effects are shortness of breath, dry mouth and headaches. Along with reduction of side effects, there is no secondhand smoke. The vapour that the user exhales quickly vanishes and does not appear to cause harm to bystanders.
A ‘quick reference guide’ for ‘smoking cessation services’, from NICE, published in February 2008 gives an overview of what was perceived then could or should be offered on the NHS to help people give up smoking. This evidence-based guidance presents the recommendations made in ‘Smoking cessation services in primary care, pharmacies, local authorities and workplaces, particularly for manual working groups, pregnant women and hard to reach communities’. It provides a rationale for who could provide smoking cessation services (as it predates the £3bn top-down reorganisation, it refers to a critical rôle for PCTs and SHAs), what pharmacotherapies might be prescribed and for whom (and where they should not be prescribed), which patient groups might be beneficially targeted, and how effectively educational and training resources might be allocated.
It is no secret that despite public health efforts the popularity of electronic cigarettes has increased at a rapid pace in recent years. E-cig sales have doubled in the last two years and they are estimated to reach $1billion in retail sales in 2013. According to a Gallup poll, 74% of smokers want to quit, and Goldman Sachs analysts believe the electronic cigarette is “the most credible alternative to conventional cigarettes in the market today”.
This investment giant estimates electronic cigarettes could reach $10 billion in sales over the next few years and account for over 10% of the total tobacco industry volume and 15% of the total profit pool by 2020. In April 2012, one of the big cigarette companies threw its hat in the ring. This was Lorillard, maker of Newport and other cigarette brands. They spent $135 million on the purchase of blu e-cigs. They’ve seen a lot of success with the brand. Sales have grown from $8 million in in the second quarter of 2012 to $57 million in the second quarter 2013. This is a gain of more than 600%. Lorillard claims they hold around 40% of the total e-cig market share. So of course Big Tobacco is eager to get in on the act, and as Hargreaves notes, cigarette manufacturers Lorillard, Reynolds American, Imperial Tobacco, British American Tobacco, and Altria are all bringing out e-cigs, along with newer companies like Vapor and privately-held NJOY.
There are, of course, risks to this growth. One realistic threat is the tightening of the manufacturing and product standards, or bring in a specific set of rules rather like those governing cosmetics. However, any government would have to be motivated to do this, and, following evidence for ‘corporate capture’ in English policy since the election of the UK Coalition government in 2010, e-cigs are likely to experience an ‘easy ride’.
But there are other considerations. Electric smokes compete with cigarettes yet do not in most places face the same restrictions, to say nothing of excise taxes. They compete with smoking-cessation products yet do not usually have to secure prior approval for products or make them to pharmaceutical standards. If they are required to do either, their price will rise, variety will fall and the uptake by consumers, who are overwhelmingly smokers, will be cut.
Furthermore, the World Health Organisation does not encourage them. America’s Food and Drug Administration is expected to propose restrictions in October. In 2009 it claimed that e-cigarettes were unapproved medical products, but a court said they should be regulated as tobacco products instead. Health authorities worldwide are struggling to deal with this new way of getting a nicotine kick. E-cigarettes are sold as leisure products and as such are covered by safety and quality standards wherever these exist and are implemented. But leaving them, like shoes or beds, to such “catch-all rules” makes some regulators uneasy. The most obvious is the involvement of the FDA. E-cig companies are anticipating that the FDA will get more heavily involved in regulating the e-cig market. This is a known risk currently being priced into e-cig dividends.
If, conversely, FDA regulation is passed, this could actually help their stock price. It would grant a degree of certainty in the minds of investors. It could also have the effect of crowding out some of the smaller players. It may also have the effect of boosting consumer confidence in the e-cigarettes. E-cigarettes, which allow users to inhale nicotine-laced vapour rather than tar-clogged smoke, are a growing market (expected to top $1billion in the next three years) but some countries including Brazil, Norway and Singapore have already banned the devices. The Medicines and Healthcare Products Regulatory Agency (MHRA) have already announced that e-cigarettes will be regulated in the UK as a non-prescription medicine. In the US, the FDA has previously warned makers for violating good manufacturing practices and making unsubstantiated drug claims.
The goal, according to Clive Bates, a former director of Action on Smoking and Health, a British campaigning group, and a tireless advocate of e-cigarettes, is not to lose the chance of millions of smokers switching in whole or in part to a relatively benign alternative. “The market is producing, at no cost to the taxpayer, an emerging triumph of public health,” he says.
In terms of the market economy, regarding the way Big Tobacco will be affected by the evolution of electronic cigarettes, Goldman Sachs predicts Lorillard will be the biggest beneficiary of the shift. after its acquisition of Blu ecigs. Blu commands 40% of e-cigarette market share and and it is expected its sales will account for 5% of Lorillard’s overall sales this year. Having a dominant e-cig brand in its portfolio puts the company in a favorable position, and could be included in even the most ‘ethical’ of pension funds in an investment portfolio.
However, perhaps the biggest threat to public health might be the market philosophy, which the current Coalition of the Conservatives and the Liberal Democrats appear to be sympathetic towards. As the Conservative Party begin their annual party conference in Manchester, it is possibly worth noting the criticism of Dr Clive Peedell, Co-Chair of the National Health Action Party, of an article by Nigel Edwards in Health Services Journal.
“In addition, market theory in the form of public choice theory rejects the idea of medical professionalism and the public service ethos. James Buchanon, “the father” of this theory admitted in a BBC documentary (“The Trap”, by Adam Curtis) that he didn’t believe in the concept of the public service ethos. Julian Le Grand famously used the “Knights and Knaves” metaphor to explain this. The solution to “rent seeking behaviour” is the discipline of the market. This would turn “pawns in queens”. The introduction of the market also explains the rise of New Public Management (managerialism), which favours narrow economic priorities and micro-management practices (e.g audit, inspection, performance indicators, league tables, monitoring and centrally imposed targets) over professional judgment [6]. (I was politicised by MMC, by the way, because I rejected its anti-professional tick box aims. It was about delivering a new breed of doctor to suit the needs of employers in the new healthcare market). And there’s more! (as Frank Carson used to say). Markets undermine the social contract between doctors and patients and damage the doctor patient relationship, because decision making becomes increasingly finance based rather than needs based. It is no coincidence that the American medical profession lost public support faster than any other profession during the rapid commercialisation of the US healthcare system in the 1970/80s.”
Libertarians might argue that citizens individually are ‘free’ to make their own choices, in the same way that ‘fat people may choose to become fatter’ due to lack of self-restraint on food. However, such crass stupidity ignores the sheer biology of how some human beings control their intake. Indeed, the first rule of recovery in substance abuse and misuse clinics in the ‘Twelve Steps’ program is for the addict to admit “powerless” over their drug of choice. Ultimately, like many of these decisions, it will come down to a cost-benefit analysis, but such sums are notoriously difficult. How much money should the NHS spend ‘from hard-working taxpayers’ money’ on such treatments, when people ‘choose to smoke’ or ‘choose to become fat’ in the rather prejudiced jaded view of the health of others? Some people might prefer this health responsibility to be offloaded who can exploit maximal rent-seeking behaviour in making a profit, in much the same way that the ‘first mover advantage’ of any Big Pharma that unlocks the secret to NHS ‘Big Data’ might become a multi-billionaire.
Deciding on the health benefits of the e-cig would have been a difficult enough job. Pile on this the consideration of this Government which knows where its priorities lie, the terrain is even more uncertain possibly.
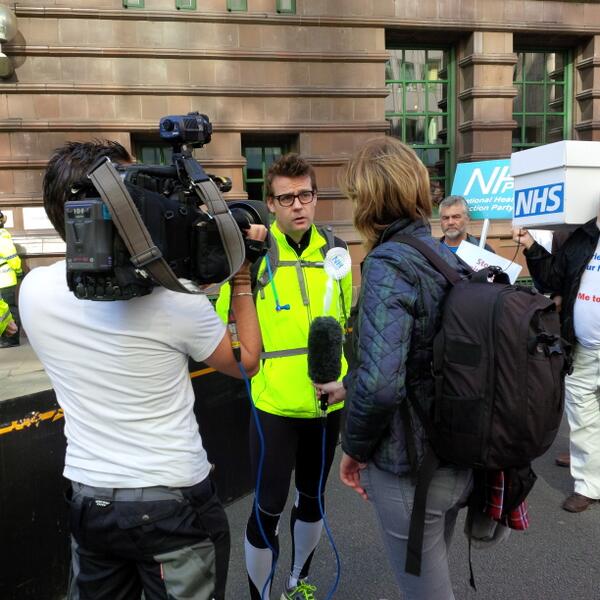
David Cameron blatantly lied to the country over NHS privatisation, says the co-leader of the National Health Action Party on the eve of his protest marathon to the Tory party conference.
Dr Clive Peedell, who’s running 42 miles on Sunday morning from the HQ of NHS England in Leeds to Manchester, says there’s incontrovertible evidence that the Coalition is privatising the NHS – despite repeated claims by the Conservatives and Liberal Democrats that their NHS reforms would not lead to increasing privatisation.
Dr Peedell, the co-chair of the NHS Consultants Association also insists that privatisation of the NHS is a false economy as it is both expensive and inefficient.
The Health and Social Care Act clearly fulfils all the commonly accepted criteria for healthcare privatisation, proving the Prime Minister has clearly misled the public, or in common language – lied.
He goes on:
If the public knew the full implications of what this would actually mean for the NHS, potential support for private provision of NHS services would plummet.
Dr Peedell argues forcefully against the assertion that it doesn’t matter who provides the service as long it’s free.
Privatisation needs a market… Market systems drain billions of pounds from the NHS budget and away from frontline care, by the creation of a huge bureaucracy of commercial contracts, accounting, legal challenges, advertising and billing.
He points out that administration costs of the NHS soared from 5% to 14% of total budget when Margaret Thatcher introduced the NHS internal market in 1991; this, he says, will increase further as “the current system is even more complex, bureaucratic and costly with three levels of bureaucracy replaced with seven”.
Dr Peedell explains that:
Private firms cherry pick the most profitable services… and leave local NHS Hospitals underfunded to pick up the pieces and deal with everything else they are expected to deal with – the full and comprehensive range of healthcare services to local communities.
And he warns that privatisation:
creates a vicious circle of increasing health care costs and financial pressure on the NHS. It leads to staff cuts, hospital and ward closures, increased waiting lists, and fewer core services provided by the NHS.
He explains how staff transfers from NHS hospitals to private hospitals (which don’t train their own staff) take vital expertise out of the NHS and how “patients have different parts of their care performed in different hospitals depending on the contracts that CCGs have signed up to. Quality is put at risk, expertise diluted, and costs driven up.”
He predicts that a failing NHS will only help boost private healthcare insurance for those that can afford it, “signalling the death knell for a universal healthcare service, free at the point of use.”
And he attacks “the revolving doors culture between the private health firms, politicians, think tanks, and civil servants within the Department of Health”.
Dr Peedell also demonstrates how the economy is damaged by the use of the private sector in the NHS:
Since public funds are used to pay for private sector provision of NHS services, taxpayers’ money is going directly into the profits of multi-national private companies and their shareholders. It is diverted away from direct patient care, and also diverted outside of our economy. Many of these companies are also registered in offshore tax havens. Privatisation of the NHS is a false economy.
In terms of political campaigning, the message that the NHS ‘reforms’ were unelected or undemocratic, and cost the ‘hard working taxpayer’ billions, is admittedly quite a good one. As political market positioning, however, this puts the #NHS in roughly the same place as an illegal war in Iraq, or a change to the GCSE examination system, or High Speed 2. It has always felt that the motivator of the ‘people being lied to’ is an apt one regarding the “democratic deficit”, and this is after all theoretically and pragmatically why millions do not vote every General Election. However, the disillusionment of voting for any political party is possibly equally divided amongst all political parties, with some more so than others, with Tory voters wondering how and why Mid Staffs and Morecambe Bay could have happened under Labour’s watch, and Labour voters wondering how the Liberal Democrats could have used weak arguments about competition law and ‘integration’ to ramraid section 75 in the House of Lords.
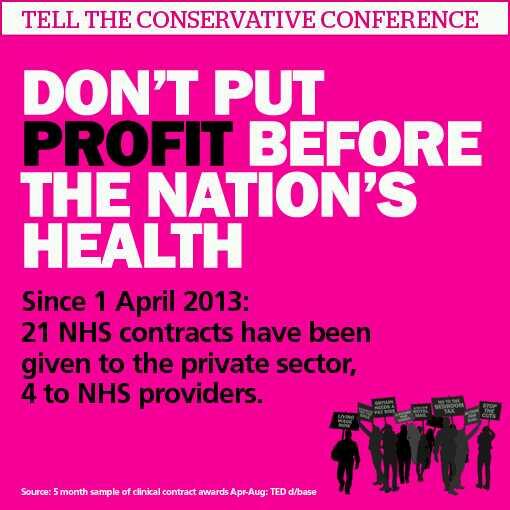
Whichever side of the fence you sit on regarding the ‘corporate capture’ of public health in this jurisdiction, whether you’re talking about standard packaging of cigarettes or minimum alcohol pricing, it is clear that the Health and Social Care Act (2012) has changed the landscape. Like an asteroid from outer space, it’s in a way intriguing how and where the Health and Social Care Act (2012) came from. Indeed, the vast majority of contracts awarded under ‘section 75’ and its equally notorious Regulations to the private sector is a testament to the efficacy of a policy which transfers resources from the public to the private sector. Part of the argument against this has been that the private sector introduces a level of repetition, waste and inefficiency substantially more than the public sector in healthcare, and the conceptualisation that there is a real ‘market’ in the NHS is an academically faulty one. A second part of the argument that this is tinkering with, to an enormous detriment, with an important societal institution of England which is held in much respect. A similar argument has been given for why Oxford and Cambridge should be given so much reverance as institutuions in the education sector and budget, when it might be more fitting that the devotion to them is manifest through the culture and heritage budget. But like Oxbridge daily, a huge number of real ‘transactions’, though perhaps not “millions”, takes place. The NHS might be a ‘sacred cow’ for some, but it is equally a powerful brand. Andy Burnham says rather mischievously that he does not wish the NHS to become, simply. a “blue and white logo”, or words to that effect, but the power of the NHS brand is illustrated that outsourcing of NHS services is done under the powerful NHS brand with massive brand loyalty.
The outsourcing of NHS services, and indeed exporting of NHS services, is part of the phenomenon where successful governments have wished to make ‘the NHS work pay’, i.e. the “hard working” NHS can pay its own way in modern England. Even better, it can ‘pay its bills’ but drawing a little salary of its own. Granted that the income might not be as huge as £20bn of Nicholson/McKinsey savings, but essentially the right wing do not like this fundamental shift of emphasis. The “change of agenda” of the NHS is prone to be dressed up as a ‘conspiracy theory’ by members of the UK Labour Party, but it is a statement of fact that the statutory purpose of directors of companies under English law is to promote the success of the company; success is defined narrowly as generating a shareholder dividend. This lends itself to the idea that private companies fulfilling NHS functions, such as domestic or multinational corporates, might be a ‘good investment’ as part of an investment portfolio, returning good profit for relatively little risk. That logic is, of course, not that daft, given that the privatised NHS market is an oligopoly, to be occupied by the usual suspects. Privatisation is inherently unpopular now with the English voting public, and the current government has put rocket boosters on a privatisation policy which has been advancing under both Labour and the Conservatives. Like energy, or broadband, despite a purported wish to ‘lower barriers to entry’ and to reward ‘value for money’ and ‘innovation’, and the usual rhetoric of Conservative memes, the contracts go to the same people, often with ongoing allegations of fraud, to deliver the same unconscionable profit for directors and shareholders for offering roughly the same ‘goods and services’ in the same crowded markets.
The ‘campaign’ against the Health and Social Care Act (2012) therefore rumbles on, and is likely to do so until the inevitable General Election to be held on May 7th 2015. Ed Miliband has successfully done what many Labour politicians have feared to do previously, and that he is: set himself the agenda, and decide to follow through his arguments. This is of course in total contrast to Lord Mandelson, who was the future once, like Lord Digby Jones, who have been fast to take to the airwaves to rubbish Ed Miliband.
But the res ipsa loquitur – this is a popular, populist policy, which has public backing, based on sound economic and legal arguments, with a clear policy motive (of delivering genuinely good value for the customer rather than high profit for a corporate). nPower has responded yesterday “a sop to Ed”, which arguably assumes that a Miliband government is a vaguely realistic possibility. Another item of evidence that a Miliband government is a realistic possibility has been the effect that this policy has had on the share price of utilities, so much so had leaks of this policy been leaked to the public ahead of the official announcement Team Miliband might have offended in civil law the use of financially sensitive information in our jurisdiction.
The damage of the ‘corporates holding the country to ransom’ narrative could be more damaging than one first expects, and this is for a number of reasons. Firstly, it is widely held, at least in political circles, that the Cameron/Clegg government is much more corporatilist than the previous Thatcher Conservative administrations, and that Cameron/Clegg have gone ‘further and faster’ than would have been possible under the likes of Thatcher, Bottomley or Ken Clarke. Secondly, the question of who drives policy is still a ‘slow burn’ issue, thanks to the successful endeavours of “38 degrees”, “Spinwatch” and “Social Investigations” (inter alia). Whilst the notion of the Unions having ‘beer and sandwiches’ is of historic interest perhaps, and indeed David Cameron would still like to whip people up into hating the unions through mechanisms such as the Lobbying Act, the mud sticking from how hedge funds appear to have called many shots in health policies is not that pleasant. This second issue of stakeholder involvement is a critical one, in that the public, even if they have horrific members of the late 1970s ‘Winter of Discontent’, have a sentiment that public sector nurses ‘do a valuable job’ and that individual membership of a Union is a democratic and laudable right.
Thirdly, the oligopoly of private provider corporates do stand, and have benefited, from the Health and Social Care Act. So this is not a question of idle speculation about privatisation – this is privatisation which is much further advanced than, for obvious reasons, Royal Mail, though the political spectacle of floating the NHS on the London Stock Exchange or AIM market is not one either main political party should currently like to entertain. Fourthly, and possibly most importantly, is the idea that the corporates on this occasion have ‘overplayed their hand’. Angela Knight, whom many people will remember for defending the behaviour of the equally uncompetitive and unpopular bankers, has been sent into battle to talk about ‘blackouts‘ and impending disaster through the short time window in which corporates can, instead, demonstrate to the rest of society that they are indeed good corporate citizens and worthy of public trust and respect. This idea of foreign-owned corporates ‘turning the lights out’ on England has of course gone down like a lead balloon, and will be in the subconscious linked to unions ‘refusing to clear rubbish up’, and so forth. The one big problem here is that Unions represent democratic bodies, but hedge funds do not.
And, finally of course, is the idea of who actually has economic, social and political power in England. Members of unions are indeed the backbone of making the NHS function (take for example UNISON’s campaigning of safe nursing staffing levels), and therefore have a legitimate say in how to ‘performance manage’ the NHS. Where frontline employee-employer relationships has been poor has been to the clear detriment of places within the service, such as the union dispute in Hinchingbrooke. The argument that there is essentially nothing wrong with transferring ‘public’ functions of the NHS to the private sector is undermined by the initial findings that David Nicholson has already had to grapple with hard-nosed issues of where competition law has been to the detriment of patient clinical care, and that any real-time underfunding of the NHS is likely to lead to backdoor rationing of services within the NHS. The ultimate merging of universal credit, ‘whole person care’ and individualised budgets could be the ultimate policy plank for any party to transfer the State duty to provide a comprehensive, free-at-the-point-of-need, universal service to one where the individual/budget holder makes his own mistakes and good budgetary decisions (and takes full responsibility for him- or her-self). As the debates about the East Coast railway and the privatisation of the Royal Mail demonstrated this week in Brighton. the idea of state-run services are popular with Union members if not with the predominantly social-democratic ‘for the public good’ members of the Labour Party leadership.
‘One Nation Labour’ can be sold, and indeed has been sold, as a doctrine where no vested interest takes control, and this is important for the three planks of Ed Miliband’s approach, economy, society and the political process. However, the NHA Party with protagonists Dr Jacky Davis and Dr Clive Peedell might equally wish to argue that the only final way to break free from this political ‘tug of war’ would be to ‘allocate your resources’ in a party focused on sorting out the NHS. They might argue that all the major parties have policy ‘blood on their hands’, e.g. the ‘private finance initiative’ proposed by Tory David Willetts in 1993, elaborated on in a major Tory thinktank in c.1997, wave of PFI contracts from Coopers and Lybrand just before Blair came to power, and further implementation of PFI under Gordon Brown and George Osborne. The concept of ‘corporates holding the country to ransom’, which the BBC and smaller media providers find hard to cope with, is an attractive one for many ‘ordinary’ voters who feel altogether disenfranchised from the political process, especially on the NHS.
If, on top of that, the notion that corporates “holding the NHS to ransom” curries favour with members of the general public ahead of how represented in the main media, Ed Miliband could find himself with the political movement on the NHS he has so long yearned for. You can already see the seeds of these theme being sown by Andy Burnham MP in his main speech to Conference in Brighton in 2013, and in subsequent copy (for example, in the Mirror or the Belfast Telegraph) that the NHS is turning into the failed system of US-style hospitals. For policy wonks, the comparison with US-style hospitals is particularly sensitive, given how Kaiser Permanente has been touted by some powerful and influential as a paradigm to follow, e.g.
Conclusion The NHS can learn from Kaiser’s integrated approach, the focus on chronic diseases and their effective management, the emphasis placed on self care, the role of intermediate care, and the leadership provided by doctors in developing and supporting this model of care.”
This is not just an issue of domestic politics, as at the moment there is no sign that the Conservative government wishes to scrutinise even the US-EU free trade agreement, regarding the ‘status’ of the NHS. The fight goes on.
Whilst many of us find the concept of the NHS being outsourced and privatised to the highest bidder quite revolting, there is also a vocal minority, with cumulatively sufficient numbers of them to hold office if not power, who believe that the Health and Social Care Act (2012) and concomitant “top down reorganisation” bring innovative, free market forces to make the NHS a “global brand leader” in the competitive world of healthcare. They believe it’s simply about making the new NHS, ‘NHS2’, “fit for purpose”, and it was only a matter of time under the two main parties (Labour and Conservative) that yet a further reorganisation of the NHS would become necessary. Arguably, the public would learn to love its benefits. Similarly, the public would learn to love HS2, “high speed 2”. Problematically, despite supportive noises from Osborne and Hammond about HS2, HS2 could still become derailed.
As the UK Labour Party hit their latest debacle of a Philip Morris stand at conference, having wished to make a stance on standard packaging of cigarettes, the tensions between populist stances maximising Labour’s electoral chances on May 7th 2015 and highly principled strategic stances based on policy have arguably never been stronger. If you’re not in Brighton for the Labour Party Conference, you might have caught sight of the “#stopHS2” campaign in the social media. Also, if you have been spending time looking at tweets about Labour’s health and social care policy, you can see the criticism of Labour over the accelerated privatisation of the NHS is not without its critics. Even intelligent well-meaning Labour supporters have been collecting electronic clippings of the continued interest in the private finance initiative (and the involvement of Coopers and Lybrand in the Major and Blair governments) and the independent sector treatment centres of the Blair government. At a time when Labour is seeking to restore faith in the political process under Lord Ray Collins of Highbury, the question that Labour is so strapped of cash that it needs Philip Morris support remains an irritating one? The notion of the ‘democratic deficit’ is seen in both HS2, as such a policy issue not even mooted in the 2010 general election which seems to have gathered cross-party support (a bit like ‘personal health budgets), and in ‘NHS2’, the top-down NHS reorganisation implemented by the Conservatives with the Liberal Democrats aiding and abetting. So if nobody voted for either policy, where did the policies from? It might not be quite the “smoke-filled rooms of beer and sandwiches”, but powerful lobbying of private commercial interests are likely to have been proven influential in the past.
Whatever the official party positions on HS2 (and this has been subject to flux in recent months), both HS2 and NHS2 have formidable national grassroot campaigns in places.Stop HS2 is the national grassroots campaign against HS2, the proposed new High Speed Two railway. Theri mission is To Stop High Speed Two by persuading the Government to scrap the HS2 proposal and to facilitiate local and national campaiging against High Speed Two.Their supporters come from a wide range of backgrounds and from across the political spectrum. The “Stop Section 75 campaign” from 38 degrees aimed at thwarting the major competitive tendering construct of the Health and Social Care Act (2012), but it was ultimately unsuccessful. 38 Degrees is the one of the UK’s biggest campaigning communities, with over 1 million members. They share a desire for a “more progressive, fairer, better society”. They tried to argue earlier this year to all MPs and members of the House of Lords that our NHS is precious – and the public overall don’t want it privatised. Privatisation for both HS2 and NHS2, here, essentially means diverting of state resources into private sector hands.
Both HS2 and NHS2 are staggeringly expensive projects in this day when we keep on having austerity rammed down our throats, but admittedly the scale of spending of each project is different. Nonetheless by anyone’s standards, £32 billion as an estimate for #HS2 is an eye-watering amount of cash. It works out at well over £1,000 for every single family up and down the United Kingdom, and large numbers of us remain unconvinced that this will be money well spent. The exact cost of the NHS2 top down reorganisation is in its own different way unclear. Following on from Labour’s claims of ‘hidden costs’ last November, Shadow Health Secretary Andy Burnham claimed that the reorganisation planned in the Government’s Health and Social Care Bill (as it was then) amounted to costs of £3.5 billion, far more than the £1.2 – £1.3 billion claimed by the Government. Minister of State for Health Simon Burns branded this figure a ‘mistake’, reasserting the Government’s own figures as the correct estimate.
Also, both policies HS2 and NHS2 are “unpopular” with the general public. This is reflected by the fact they have never been openly discussed with the public before implementation. The public remain unconvinced about the actual rationale for HS2 to bring greater equity between London and regions of England (critics argue that the plan would benefit London more than the regions). Likewise, at a time when the ‘cost of living’ has been thrust into pole position by Ed Miliband, the cost of non-NHS providers providing NHS products and services for a cost which enhances shareholder dividend, the case for pimping out the NHS to the private sector has never been more badly timed. A YouGov poll into spending cuts commissioned by the TaxPayers’ Alliance last summer found that 48 per cent of people supported cancelling plans for HS2, with barely a third wanting to press ahead with the scheme. And it’s hardly surprising that the public remains so reluctant to support it. Andrew Lansley’s NHS reorganisation is unpopular both with the public and health service staff. Such a large scale reorganisation (likened to “throwing a grenade into the NHS”, by Conservative MP Dr Sarah Wollaston) would be difficult even in the Blair years of increased funding.
Research published by the TaxPayers’ Alliance last year into the hidden costs of HS2 further set alarm bells ringing, highlighting, for example, the billions of additional funding that would be necessary to mitigate the environmental effects of the line by running more of it underground or through tunnels. Andy Burnham, Shadow Health Secretary, spoke of a “bruised and battered” NHS that was in a “fragile” state. Burnham believes there is now a choice to be made about whether we want to allow the inexorable advance of competition in the market, or whether we want to hold on to a planned national system that many successive generations in England have benefited from.
Both HS2 and NHS2 pose fundamental problems for the Labour policy review, still currently underway. They poses problems for the UK economy – how much benefit are we actually going to get from this surge of spending to implement them? They also pose problems for the public’s institutions. Both the railway network and the NHS are cherished by the public but in different ways. Many citizens, whether they are Labour voters, think that the privatised railway industry has become costly, fragmented and essentially a shambles following Tory privatisation, and some would fundamentally like it in state ownership. While Burnham has consistently said the dichotomy between public and private is a false dichotomy, he has also reiterated his affirmation for the ‘NHS preferred provider’ policy which is a small attempt to mitigate against the loss of a state-run comprehensive universal National Health Service.
Both HS2 and NHS2 are ‘elephants in the room’, and it is merely a question of time for how long they may remain hidden.
In the beginning, there was garbage and rhetoric. It sounded nice, but it was intellectually devoid of quality, there was not much competition for ideas even though this WAS bad, and so there was not much choice.
Julian LeGrand back in 2003 talks of the “competition juggernaut”:
Labour has made many mistakes, usually and unsurprisingly given its roots in socialism and central planning, in the direction of too heavy-handed central control. The public service juggernauts are now on a different course, with decentralisation, competition and choice as part of their route maps – and with plenty of resources as fuel. If they fail to arrive at their destination, if our expectations are dashed, there will be real questions over the future of each area of public services: how long can it remain public; how long can it remain a service?
‘Competition fever‘ should have never have got off the ground. The University of York, Economics of Social Care and Health Unit, and Centre for Health Economics once published a study of ‘Hospital competition under fixed prices’ (research paper 80).
The argument that competition improves quality fell apart because of the sheer volume of invalid assumptions, as demonstrated in the following quotation from that document:
The review of the theoretical literature suggests that the plausible argument that greater competition amongst providers facing fixed prices will lead to higher quality rests on strong assumptions which may not hold. The literature shows that more competition increases quality when providers are profit maximisers and marginal cost of treatment is constant. Competition has an ambiguous or negative effect on quality when providers are altruistic, the marginal cost of treatment is increasing and quality is only imperfectly observable. The literature has been largely silent on the relationship between market size, as measured by total population or population density, and quality.
Competition as the failed central plank of the Health and Social Care Act (2012)
The raison d’être of the Health and Social Care Act (2012) is nothing to do with improving clinical care, though that could be a consequence of its three main areas. There is nothing about how patient staffing can be addressed, related to the equally potent issue of patient safety. It has never been entirely clear how the Act came about, but the three planks of policy are laid bare by the impact assessments from the Department of Health (2011) (published here on 19 January 2011). The three main planks of the Bill are firstly to establish the competitive market as the substrate for the National Health Service, to define better the insolvency régime (it is important to clarify how economic entities as autonomous units can be allowed to fail ‘to get them out of the system’), and the machinery needed to regulate the market. I will come to how Monitor has had to come into being to ‘regulate the internal market’, but it is not insignificant that introducing the market is itself a source of waste and inefficiency (such as duplicated transaction costs). Of course, the issue of how to regulate the internal market should be regulated has often been analysed in a substandard manner before by some social scientists, not competition lawyers, but this is now an important policy issue which has been thrust into the limelight.
Central to this argument is that competition promotes innovation. This is indeed cited on page 41 of the “Impact assessment”.
Ahn (2002) reviews a large number of studies on the link between competition and innovation and concludes that competition encourages innovative activities and has a significant impact on long-term productivity growth:
“Competition has pervasive and long lasting effects on economic performance by affecting economic actors’ incentive structure, by encouraging their innovative activities, and by selecting more efficient ones from less efficient ones over time”.
The myth that competition drives innovation, when COLLABORATION does
However, there is an intrinsic problem in business management: the assumption that competition drives innovation. This bit of missing evidence in the impact assessments totally distorts the raison d’être of the Act itself, and of course there is a separate debate in management as to whether innovation can be detrimental to organisational culture or learning. There is considerable evidence now that collaboration, not competition, can be essential for innovation. This theme is taken up in an interesting article about ‘internal markets’ from Forbes:
Major innovation needs collaboration, not competition. For innovation, internal markets have the same problem as hierarchical bureaucracies. Managers vote their resources for innovations that bolster their current fiefdoms and careers. The safest strategy is to stick to the status quo. Ms. Kimes’ article gives multiple examples where competing managers at Sears looked after their own units at the expense of the interests of the firm as a whole.
Second, innovation isn’t basically an issue of spending. Booz & Company’s annual innovation reports repeatedly state: “Spending more on R&D won’t drive results. The most crucial factors are strategic alignment and a culture that supports innovation.”
Finally, the hope of the internal markets theory is that, by funding a variety of different ideas, the organization will emulate the evolutionary process of natural selection and so the best ideas will survive and prosper. The problem is that once a disruptive idea starts to flourish and becomes more interesting than the normal bread-and-butter work of the organization, it risks becoming a threat to the rest of the organization.
The wheels are coming off the Competition Juggernaut a bit sooner than expected
David Williams at the Health Services Journal only very recently on 16 September 2013 reported that:
NHS England has delayed the publication of its choice and competition framework amid a “paucity of evidence” of the benefit to patients.
Policy director Bill McCarthy made the announcement at a board meeting on Friday, highlighting the issue as a new risk for the central body.
The framework and supporting documents were originally slated for publication in July.
Mr McCarthy said: “We’re having [a discussion] with Monitor around choice and competition, and how best they can be applied in healthcare to improve outcomes for patients, including a better experience.
“That’s taken a bit longer than we hoped.
“We had hoped to be able to put out some guidance early in the summer – I think that probably reflects… it is one of the areas where there is a paucity of evidence.”
“Operation Propper”
Clause “B47” (p.42/3) in the official Impact Assessments from the Department of Health cites one of the key planks of evidence that the Department of Health wishes to use in promoting its competition argument.
“A July 2010 study by health economists Martin Gaynor, Rodrigo Moreno-Serra, and Carol Propper investigated outcomes in the NHS following the introduction of choice in 2006. They conclude as follows: “We find that the effect of competition is to save lives without raising costs. Patients discharged from hospitals located in markets where competition was more feasible were less likely to die, had shorter length of stay and were treated at the same cost”. The study found that there was a larger inflow of patients to better quality hospitals after the 2006 NHS reforms, suggesting that popular providers in health care are able to expand supply.”
There is an even worse justification for the competition dogma later in the Department of Health’s official impact assessments:
B48. A January 2010 study by the London School of Economics also looked at NHS data post- introduction of choice in 2006. The key conclusion is as follows: “Using AMI mortality as a quality indicator, we find that mortality fell more quickly (i.e. quality improved) for patients living in more competitive markets after the introduction of hospital competition in January 2006. Our results suggest that hospital competition in markets with fixed prices can lead to improvements in clinical quality”.
B49. Evidence from the LSE shows that management quality – measured using a new survey tool – is strongly correlated with financial and clinical outcomes such as survival rates from emergency heart attack admissions (AMI). Moreover, the study finds that higher competition (as indicated by a greater number of neighbouring hospitals) is positively correlated with increased management quality.
The major improvements in outcome after acute myocardial infarction can be attributed to improvements in primary prevention in general practice and in hospital care, including the introduction of percutaneous IV angiography. The government’s own cardiac Tzar, Sir Roger Boyle, was sufficiently angered by their claims to respond with withering criticism: “AMI is a medical emergency: patients can’t choose where to have their heart attack or where to be treated!” It is “bizarre to choose a condition where choice by consumer can have virtually no effect”. Patients suffering “severe pain in emergencies clouded by strong analgesia don’t make choices. It’s the ambulance driver who follows the protocol and drives to the nearest heart attack centre”.
The intervention that the authors claimed reduced heart attacks and was a proxy for competition was patient choice. In 2006, patients were given choices of hospitals including private for-profit providers for some selected treatments. Less than the half patients surveyed in 2008 even remember being given a choice, and only a tiny proportion made those choices based on data from the NHS choices website. If patient choice was one of the two key elements of competition, it wasn’t prevalent and rather than being derived from the authors’ data, it was assumed.
Crucially, even if patient choice had occurred it does not explain why heart attack mortality rates fell. There is no biological mechanism to explain why having a choice of providers for elective hip and knee operations surgery (including hospitals which did not treat or admit acute MI patients) could affect the overall outcomes from acute myocardial infarction where patients do not exercise choice over where they are treated.
The problem of data dredging is well known; if you repeat an analysis often enough significant statistical associations will appear. But the authors make the cardinal error of not understanding their data and of confusing minor statistical associations with causation. Deaths from acute MI are not a measure of quality of hospital care, rather a measure of access to and quality of cardiology care. At best, what the paper appears to show is not the effect of choice on heart attacks but that if an individual has a heart attack in an area close to a hospital and their GP is near the hospital, then outcomes are better, but such findings are not new.
Going for their central criticism, in the same article, they explained:
The drip feed of pro-competition studies from Zack Cooper at LSE raises serious questions for the academic community and the public about what constitutes bad science and what to do about its politicisation. Recently, on 21 February in the columns of the FT, Cooper and colleague Julian Le Grand warded off serious scientific criticisms of the studies with an ad hominem attack, categorising those in favour of competition as empiricists and those whose work is critical of markets in health care as intuitivists. In so doing they sweep aside decades of careful economic theory and evidence which shows why markets do not work in health services and distract the reader from the facts that their work is ungrounded and far from empirical. Their repeated claims that competition in the NHS saves lives and improves quality and productivity have no scientific basis.
A litigation factory?
Of course the £3bn Health and Social Care Act (2012) which have no mechanisms of helping with clinical staffing or patient safety, in the drive for business efficiencies, have become a bonanza for private companies to which work has been outsourced, and a boon for the commercial and corporate law firms which are now nurturing them. The NHS of course has trouble in meeting the formidable legal bill against the private providers, as well as staff it has made redundant due to this top-down reorganisation.
I have long argued that the commissioning (‘competition and choice’) process through section 75 Health and Social Care Act (2012) would soon turn sour, for example in the original blogpost I did for the Socialist Health Association in January 2013 here. Crispin Dowler recently reported early tensions on 11 September 2013 in the Health Services Journal:
A number of private providers are likely to take complaints to the NHS’s new competition regulator Monitor over the next three years, the chief executive officer of Ramsay Health Care UK warned last week.
Jill Watts, whose organisation was ranked the largest private provider of NHS funded acute care in the most recent study by market analysts Laing and Buisson, said she could “almost guarantee” there would be challenges to come.
She told a Westminster Health Forum conference that the April switchover to clinical commissioning groups under the government’s health reforms had not produced uniform changes in commissioners’ attitudes to the private sector.
“In one part of the country, where we had almost adversarial relationships and they didn’t want to use us at all, they’re very keen to work with us now,” she said.
The New Labour Legacy, competition, performance and “the target culture”
Competition was intimately wound up in the target-driven agenda. NHS hospitals would have to meet targets to jump through regulatory hoops to become NHS Foundation Trusts. As long as finances stacked up, patient safety appears to have suffered in some Trusts under Labour’s watch. Whilst the evidence for competition being beneficial in the NHS market is weak, it has remained with us in policy like a bad smell. Julian LeGrand could have not put better how idiotic this policy really was.
The problem is indeed partly money – a historical legacy of underspending in all areas of public services. But, as John Hutton says, it isn’t only that. There is also a legacy of poor performance: of failing to use what resources there are effectively and efficiently. This is a lesson that six years in power have taught New Labour. The Government has tried and is trying a wide variety of techniques to lever up performance: publishing league tables on comparative performance, encouraging private sector involvement, offering independence to high fliers, stimulating competition and choice. But one of its favourite instruments has been targetry: the setting of targets with heavy penalties for failing to meet them. Many in government are convinced that this is the way to go.
According to a recent newspaper article, the latest workforce statistics obtained by Nursing Standard magazine from the Health and Social Care Information Centre reveal that there are 348,311 nurses, midwives, school nurses and health visitors working either full-time or part-time in England. That is 2,991 fewer full-time posts than when the coalition government came to power. United Lincolnshire Hospitals NHS Trust, Basildon and Thurrock University Hospitals NHS Foundation Trust and Burton Hospitals NHS Foundation Trust are “plugging gaps” by hiring nurses from abroad. Basildon and Thurrock is looking to recruit 200 nurses from the Philippines and Spain. The international campaigns launched by the trusts reflect a growing trend to search beyond the UK for staff.
According to reports from Whiston, management staff have defended their recruitment policy after it transpired that Whiston Hospital’s A&E was understaffed by around eight per cent. An investigation by the BBC found that 11 of the 131 positions at the hospital’s casualty department remained unfilled. It is believed the shortfall is regularly made up by employing bank and agency staff, in line with other reports from around the country. The revelations about staffing levels, made following a Freedom of Information Act request, have unsurprisingly prompted nursing leaders to criticise current staffing levels. Meanwhile, according to reports from Croydon, a staffing crisis at Croydon University Hospital A&E has left it with the second largest shortfall of permanent employees in the country. That ward has a third fewer permanent workers than its NHS trust believes it needs, with the biggest gap in the supply of nurses. Croydon Health Services NHS Trust employs 151 permanent A&E staff, a shortfall of 48. Only Barking, Havering and Redbridge University Hospitals NHS Trust had a bigger deficit of staff, according to official statistics obtained through Freedom of Information requests. The trust stressed holes were plugged with temporary and agency staff, although these typically cost more than full-time employees. It claimed employing temporary staff did not impact on standards of care, unsurprisingly.
Last week, the Royal College of Physicians published its “Future Hospital Commission” report (“Report”). Generalist and specialist care in the future hospital came under some scrutiny in this report, but not in a way which addresses where there can possibly be more Doctors ‘on the ground’. Generalist care includes acute medicine, internal medicine, enhanced care and intensive care. Specialist components of care will be delivered by a specialist team who may also contribute to generalist care. A critical question is, in the average DGH, which of the ‘specialists’ are going to chip in with the acute general medical take. Currently, it is not uncommon for respiratory, gastroenterology and endocrinology physician consultants to run the acute general medical take, but (generally) neurologists and cardiologists do not take part.
“Patients should receive a single initial assessment and ongoing care by a single team. In order to achieve this, care will be organised so that patients are reviewed by a senior doctor as soon as possible after arriving at hospital. Specialist medical teams will work together with emergency and acute medicine consultants to diagnosis patients swiftly, allow them to leave hospital if they do not need to be admitted, and plan the most appropriate care pathway if they do.”
The “24/7” aspect of ‘Future Hospitals’ is emphasised in various places in the report, for example:
“Acutely ill medical patients in hospital should have the same access to medical care on the weekend as on a week day. Services should be organised so that clinical staff and diagnostic and support services are readily available on a 7-day basis. The level of care available in hospitals must reflect a patient’s severity of illness. In order to meet the increasingly complex needs of patients – including those who have dementia or are frail – there will be more beds with access to higher intensity care, including nursing numbers that match patient requirements. There will be a consultant presence on wards over 7 days, with ward care prioritised in doctors’ job plans. Where possible, patients will spend their time in hospital under the care of a single consultant-led team. Rotas for staff will be designed on a 7-day basis, and coordinated so that medical teams work together as a team from one day to the next.”
Against this is the backdrop of the Nicholson “efficiency savings”, as reported (for example) here in the Guardian:
“The prime minister, David Cameron, his health secretary, Andrew Lansley, and the NHS’s most senior figures have all stressed that the government’s drive to make £20bn of efficiency savings in England by 2015 should not prompt hospitals and primary care trusts to cut services provided to patients. Instead, they say, the money should be saved through reducing bureaucracy, ending waste, adopting innovative ways of working and restructuring services.
Yet the growing evidence from the NHS is that its frontline is being cut, and that NHS organisations are doing what they were told not to do – interpreting efficiency savings as budget and service cuts. While restricting treatments of limited clinical value – such as operations to remove unsightly skin – is uncontroversial, reducing patients’ access to drugs, district nurses, health visitors or forms of surgery they need to end their pain arouses huge concern.”
Shaun Lintern, in a typically excellent article in the Health Services Journal, threw some light on this in relation to the report by Professor Sir Bruce Keogh, in July 2013:
“The NHS has little idea whether staffing levels at English hospitals are safe, Keogh review panel members have admitted. The report by NHS England medical director Sir Bruce Keogh said data for eight of the 14 hospital trusts examined by the review suggested there was no problem with nursing levels on wards.But when the review teams carried out their inspections they found “frequent examples of inadequate numbers of nursing staff in some ward areas”. In his report Sir Bruce said: “The reported data did not provide a true picture of the numbers of staff actually working on the wards.” The review suggests high level data on workforce levels may present an unrealistic impression of staff available on hospital wards on any given shift. This could lead to NHS trusts drawing false assurances from workforce data while their wards go understaffed. At several of the trusts examined the review team found staff feeling unable to voice their concerns to senior managers.”
Julie Bailey and #CuretheNHS, as well as a number of prominent patient groups such as #PatientsFirstUK, as well as certain regulatory authorities such as the #CQC, have all emphasised the need for ‘safe staffing’ for the NHS to succeed. Prof Sir Brian Jarman has time-and-time-again emphasised the pivotal impact of safe staffing on the hospital standard mortality ratio, as for example in this seminal article from the BMJ in 1999, on page 1517:
“In model A higher hospital standardised mortalityratios were associated with higher percentages of emergency admissions, lower numbers of hospital doctors per hospital bed, and lower numbers of general practitioners per head of population. The numbers ofhospital doctors of different grades were also considered as explanatory variables, but total doctors per bed was found to be the best predictor.”
A symptom of a poorly staffed NHS (in certain autonomous units) would be the system completely falling apart from the strain of increased numbers during the Winter period. A ‘solution’ proposed by NHS England has been some of £2.4 billion surplus will be plugged into a ‘quick fix’ of the situation, and/or hospitals can employ temporary bank staff. This may in the short term attempt to mitigate against a dangerous situation. According to the GMC(UK)’s “Good medical practice” (at point 56):
“56. You must give priority to patients on the basis of their clinical need if these decisions are within your power. If inadequate resources, policies or systems prevent you from doing this, and patient safety, dignity or comfort may be seriously compromised, you must follow the guidance in paragraph 25b.”
Many senior consultants do not wish to speak out safely currently against poor resources. This is reflected in this tweet/comment by Dr Kim Holt:
This further emphasises the need for (all) staff to speak out safely against dangerous clinical care (hence the critical importance of the “Nursing Times Speak Out Safely” campaign.) From the consultant physician front, with the ‘input’ from operations and flow managers, there are currenltly reports of insufficient doctors and nurses being able to see patients in A&E in a timely fashion. It seems that the response to this, while NHS managers have remained consistently immune from materially significant blame for poor clinical care, has been for medical consultants to shunt patients, including vulnerable frail patients, out of A&E into MAU (or even, at worst, medical outlier wards), without patients having ever been clerked. That would be therefore direct evidence of a ‘gaming’ managerial culture directly impacting on how NHS consultants on the ‘shop floor’ have to react in the face of cuts and pressures from clinical demand. Whilst it might be sexy for all politicians and the Royal College of Physicians of London to talk about 24/7, no government minister has gone public to say how they will literally achieve ‘more for less’. Where will the extra money come from? Presumably existing staff will have to do more work for the same pay, and still have to comply with the law governing working (i.e. the Working Time Regulations passporting the European Time Directive).
Whilst their Report is to be welcomed, the Royal College of Physicians have effectively delivered a ‘motherhood and apple pie’ document for Government. It sounds nice and does not even address issues relating to the home patch? One of them will be for the Council of the College to consider whether it wishes for ‘specialist’ Consultants to ‘chip in’ with the acute medical take 24/7. They have after all at some stage passed the Diploma of the Royal Colleges of Physicians (UK)?
Meanwhile, for all the methodological criticisms of Jarman’s work, it can only be assumed that he genuinely wishes to improve the quality of care of NHS hospitals in England, and that he sincerely wishes to prevent the staggering distress of those foci of poor care where evidenced previously in the NHS. His words, on @RoyLilley’s “NHSmanagers.network” blog, could not have been clearer.
The fiasco over the HSMR is now of totemic proportions.
In many ways, the battle over the Channel 4 headline story of Wednesday saying “for the first time” that hospital mortality rates in the UK were considerably higher than other jurisdictions has become more totemic than the notorious “War over Jennifer’s Ear“. To give him credit, Prof Brian Jarman (@Jarmann) is always very helpful on Twitter. There can be a temptation to play the man not the ball, but Jarman has a very distinguished professional record as a member of the medical profession as part of the St. Mary’s Hospital/Imperial College centres in London. By his own admission, his first degree was in physics, and his PhD on Fourier analysis of seismic wave propagation. He changed to medicine age 31. There is absolutely no doubt that Prof Brian Jarman is an incredibly bright man. On the basis of presumption of innocence under English law, it is critical to assume that Prof Jarman did not intend to mislead the general public through the reporting of his claims over hospital mortality statistics. This is indeed consistent with the positioning of excellent patient safety campaigning groups who overall feel that a discussion over the statistics is a genuine offense to the misery of relatives (and families) who have suffered. There is perhaps an issue of whether Jarman was particularly reckless in how such data might be presented before a fearful public, and possibly how Jarman’s data are presented in the media, following the Telegraph and similar reports and this week’s Channel 4 presentation, in the future might be the best surrogate guide to Jarman’s true intentions.
The Channel 4 website report, “NHS hospital death rates among worst, new study finds“, is here.
“NHS chief Sir Bruce Keogh says he is taking very seriously figures revealed by Channel 4 News which show that health service patients are 45 per cent more likely to die in hospital than in the US.”
According to this Channel 4 website report:
“The figures prompted Sir Bruce Keogh, medical director of the NHS, to say he will hold top-level discussions in a bid to tackle the problems. I want our NHS to be based on evidence. I don’t want to disregard stuff that might be inconvenient or embarrassing…I want to use this kind of data to help inform how we can improve our NHS,” he told Channel 4 News.I will be the first to bring this data to the attention of clinical leaders in this country to see how we can tackle this problem.”
2. The methodology of the “hospital standardised mortality ratios” (HSMRs)
Jarman’s ‘discovery’, in a flourish worthy of ‘Gone with the Wind’ perhaps, is described thus:
“What he found so shocked him, he did not release the results. Instead, he searched – in vain – for a flaw in his methodology and he asked other academics to see if they could find where he might have gone wrong. They, too, could not find fault.”
The question remains: what happened in the intervening nine years which prevented any activity culminating in professional peer review?
3. These data were indeed presented as far back as 2004
The Channel 4 reporting was sensational as illustrated in this excerpt from the Channel 4 report by Victoria Macdonald:
“So now he is releasing the findings. And they are shocking. The 2004 figures show that NHS had the worst figures of all seven countries. Once the death rate was adjusted, England was 22 per cent higher than the average of all seven countries and it was 58 per cent higher than the best country.”
The data are even known to the Department of Health as evidenced by Jarman himself here:
The starting point of the report was to go to the Mayo Clinic:
“Because of confidentiality issues we are not allowed to name the other countries. But America stands out in the data for its lower mortality rates. So we went to find out why. At the Mayo Clinic Hospital in Phoenix, Arizona, they are in the best two per cent in the country. It is an impressive hospital, with piano music playing in the lobby and sunshine streaming into the rooms.”
4. Concerns about the data
Any (reasonable) reviewer of these data, particularly given the bold and significant nature of the claims therein, will be concerned about the ‘quality’ of the data, in much the same way Jarman is concerned about the ‘quality’ of healthcare. This is particularly so if one adopts the approach of ‘treating the data’ rather than ‘treating the clinical patient’, which many clinicians would not advocate anyway in isolation.
This ‘confidentiality issue’ about the manner in which these data were provided is confirmed in a recent tweet by Jarman:
In the absence of clarity of what these confidentiality issues precisely are, it is hard to deduce fully what it is exactly that is so prohibitive for Jarman publishing his data. Many senior academics indeed converge on the notion that the publication of these data would be a useful contribution to the field, provided that the publication were properly refereed from two perspectives. These perspectives are that the statistical techniques used are sound. The second perspective is from a clinician’s perspective that the correct public health policy issues have been identified, and analysed correctly using available global evidence, and the citation of relevant background assumptions and confounding factors. Whilst it is hard to conceive that Governments have been withholding publication of data on public policy grounds (and arguably there is no more important a policy issue than a country’s mortality), it is possible that individual private companies may not wish to disclose fully confidential data. In the private sector even, such lack of disclosure of confidential data has led to accusations of fraud and discussion of mitigation, because of the sensitivity of such data to the markets in the dividend signalling theory. Academics have suggested to Jarman on Twitter that it might be possible to publish these data using the techniques of anonymisation or pseudo-anonymisation, as is prevalent in contemporaneous scientific research, but again no answer has been readily provided.
5. The utility (and futility) of cross-jurisdictional comparisons
The financial situation of the Mayo Clinic itself is known to be strong, with a colossal amount of income per patient at the Mayo Clinic compared to a patient in the English National Health Service:
“But a copy of the clinic’s consolidated financial report obtained by the Pioneer Press shows total revenue of $8.48 billion in 2011. That was an increase of $533 million, or nearly 7 percent over revenue of $7.94 billion during the previous year. Income from operations increased by 18 percent, growing from $515.3 million in 2010 to $610.2 million last year, according to the financial report. “This is very strong,” said Steve Parente, a professor of finance at the University of Minnesota’s Carlson School of Management. “In terms of pure operations, they’re doing quite well….Their grants and contracts are going up, too,” said Parente, who reviewed the financial report.””
A pertinent issue is whether the hospital episode statistics are themselves reliable. Prof Jarman quoting other reports feels that they are reliable (see tweet). However, this is in contradistinction from other reports sourced at the Royal College of Physicians of London (as described in a previous Guardian article):
“Currently the public can use the NHS Choices website to help them choose a hospital for treatment. NHS Choices, and the information used by Dr Foster, is based on “Hospital Episode Statistics” (HES) data, which the NHS says is “authoritative and essential”. However, NHS insiders say the information, usually collected by administrative staff from patient records, is unreliable.Professor John Williams, director of the health information unit at the Royal College of Physicians, carried out a study into HES data and found a significant number of operations were recorded inaccurately. He has called for a change in the way data is collected, saying flaws in the HES database were exposed as long ago as 1982.”
Hospital death rates, particularly if followed over time, can give useful warning of problems, as Sir Bruce Keogh has stated. Dr Jacky Davis in a subsequent Channel 4 interview (see below) was asked about the ‘smoke detector’ use of HSMRs as being pivotal in warning about problems.
It is, for example, argued that the issues in Mid Staffs would not have been exposed, but for the HSMRs. This argument is relatively convincing, but it is also argued that any reader of the local papers in Mid Staffs would have been aware of the problem long before the official HSMR figures emerged. Dr Jacky Davis in her C4 interview on Thursday, in reply, admitted that this ‘smoke detector argument’ might be true, but explained further ‘if there’s smoke going up you have to make sure – is there a fire there?‘. This is intuitively true, as well as the notion that the mortality rate in any given hospital will depend on the numbers of people who are actually dying ‘on site’. In general of course variation of data in other jurisdictions are likely to relate to regional variation of the care of palliative care patients, for example, and also where the funding for medical care is coming from (for example, the location of death may be an artifact of the conditions of private insurance funding.)
However, arguably reliable comparison of such data internationally is fraught with difficulties, as Prof Walter Holland and colleagues found out when they published the European Atlas of Avoidable Deaths in 1988. Prof Holland is an eminent expert in public health and a visiting Chair at the London School of Economics. Since total mortality rates in the UK are similar, or lower, than in the United States, as a large proportion of the population in both countries die in a hospital such a difference seems unlikely, according to Holland. To compare hospital mortality rates between hospitals, whether in one or more countries, arguably it is necessary to take into account such factors as availability of discharge facilities, e.g. hospices, hospital admission criteria, length of time in hospital, and many other procedural and cultural factors, according to the eminent Holland.
“Our findings suggest that the current Dr Foster Unit method is prone to bias and that any claims that variations in standardised mortality ratios for hospitals reflect differences in quality of care are less than credible.812 Indeed, our study may provide a partial explanation for understanding why the relation between case mix adjusted outcomes and quality of care has been questioned.24 Nevertheless, despite such evidence, assertions that variations in standardised mortality ratios reflect quality of care are widespread,25 resulting, unsurprisingly, in institutional stigma by creating enormous pressure on hospitals with high standardised mortality ratios and provoking regulators such as the Healthcare Commission to react.20“
In our jurisdiction, for example, the proportion of surgery done as elective day cases is reported to be quite high. Unfortunately the data presented by Jarman in his original 2004 presentation and the Wednesday Channel 4 package are inadequate alone for anyone to determine the validity of the conclusions or the methods used. This is a striking media story but unfortunately has not been subjected to proper scrutiny. This will be essential for policy in English health policy, particularly in the critical issue of patient safety, to progress; and progress it must not on the basis of emotion or soundbites.
6. A wider issue
Prof Jarman has consistently stated that he is in favour of a NHS funded by taxation, which is different from the attitude of libertarians and the Mayo Clinic, as shown here:
Critics of Jarman have felt that his criticisms of some foci of the delivery of care undermine the daily work of clinicians across the country, and may even undermine the doctor-patient relationship so pivotal for the work of clinicians in real life (see for example here).
Jarman and supporters feel, however, that for ages criticisms of poor quality of care in the NHS have been suppressed, and that there is a professional duty to speak up about such poor care to improve the NHS. However, critics of Jarman feel that such an approach ‘in the wrong hands’ is merely providing ammunition for further marketisation and privatisation of the NHS, and that Jarman is carrying out the ‘handy work’ for politicians to see this ideological goal come into fruition.
This debate is intense with accusation and counter-accusations, but the volume of criticism regarding the NHS article headlining Channel 4 news on Wednesday is a testament to how the public will not accept unqualified comparisons of the NHS with other jurisdictions either. The ensuing analysis has further put the spotlight on Jarman’s data, but this can be no bad thing either. The medical and nursing professions, and their regulatory bodies, will wish for all involved to maintain the reputation, trust in and confidence in their work, but this is only possible if the work is ‘fit for purpose’. Politicians can slag off the NHS to an extent to which clinicians would likely become disciplined for, and it is this contradiction which raises eyebrows.
7. Conclusion
Notwithstanding, it is clear that the fundamental mistake is that it was perceived by some that the Channel 4 report represented irresponsible journalism in that the assumptions were not accurately stated, it suffered from bias by omission by lack of explanation about the surrounding issues (not least presenting Keogh as somebody who tacitly endorsed the uncritical issue of the HSMR, which is false), and basically left a very ugly taste in many people’s mouths. It did no favours for the reputation of, trust in, and confidence in Channel 4 news reporting either that night (Wednesday), but in fairness to Channel 4 news they hosted an interview with @DrJackyDavis – Co-Chair of the NHS Consultants Association – the following evening (Thursday).
However, it is impossible to deny the value of the discussion which has ensued after this dreadful report. The policy situation is precarious, aggravated by certain Ministers of the Crown lying blatantly in the whole saga over a period of months in the current Government.